Medical disclaimer: This article is for educational purposes only and does not constitute medical advice. If you have diabetes, prediabetes, or take glucose-lowering medications, please consult a qualified healthcare professional before altering your diet, exercise routine, or supplement regimen.
Stable blood sugar is one of the most reliable indicators of robust metabolic health. It is also one of the most actionable and reversible drivers behind chronic fatigue, stubborn weight gain, and long-term cardiovascular risk. According to the Centers for Disease Control and Prevention (CDC), more than 1 in 3 U.S. adults have prediabetes—and the vast majority are completely unaware.
The lifestyle inputs that slowly build insulin resistance and prediabetes—such as heavy reliance on refined carbohydrates, sedentary routines, chronic sleep deprivation, and late-night snacking—are the exact same factors that trigger daily energy crashes and relentless brain fog.
This comprehensive guide translates the complex science of glucose and insulin into a highly practical, day-to-day playbook. It expands upon the foundational concepts introduced in our Metabolic Health Guide, the cellular mechanisms explored in How Metabolism Works, and the circadian rhythms detailed in our Sleep Schedule Reset Guide.
Quick Summary (TL;DR)
- The Baseline: In a healthy metabolism, post-meal glucose rises slightly and returns to baseline within 2–3 hours. Insulin resistance occurs when your cells stop responding efficiently to insulin, forcing the pancreas into overdrive—a direct precursor to type 2 diabetes.
- The Biomarkers: Focus on three core metrics: fasting glucose, HbA1c (your 3-month average), and CGM time-in-range. Adding fasting insulin or HOMA-IR can catch metabolic dysfunction years before your fasting glucose naturally drifts upward.
- The Strategy: The highest-leverage actions are prioritizing a fiber-rich diet, combining aerobic and resistance exercise, practicing early-day eating, securing 7–9 hours of sleep, and achieving modest weight loss if necessary.
- The Extras: Natural supplements like berberine and cinnamon offer marginal benefits but cannot replace the foundational pillars of diet, exercise, and prescribed clinical treatments.
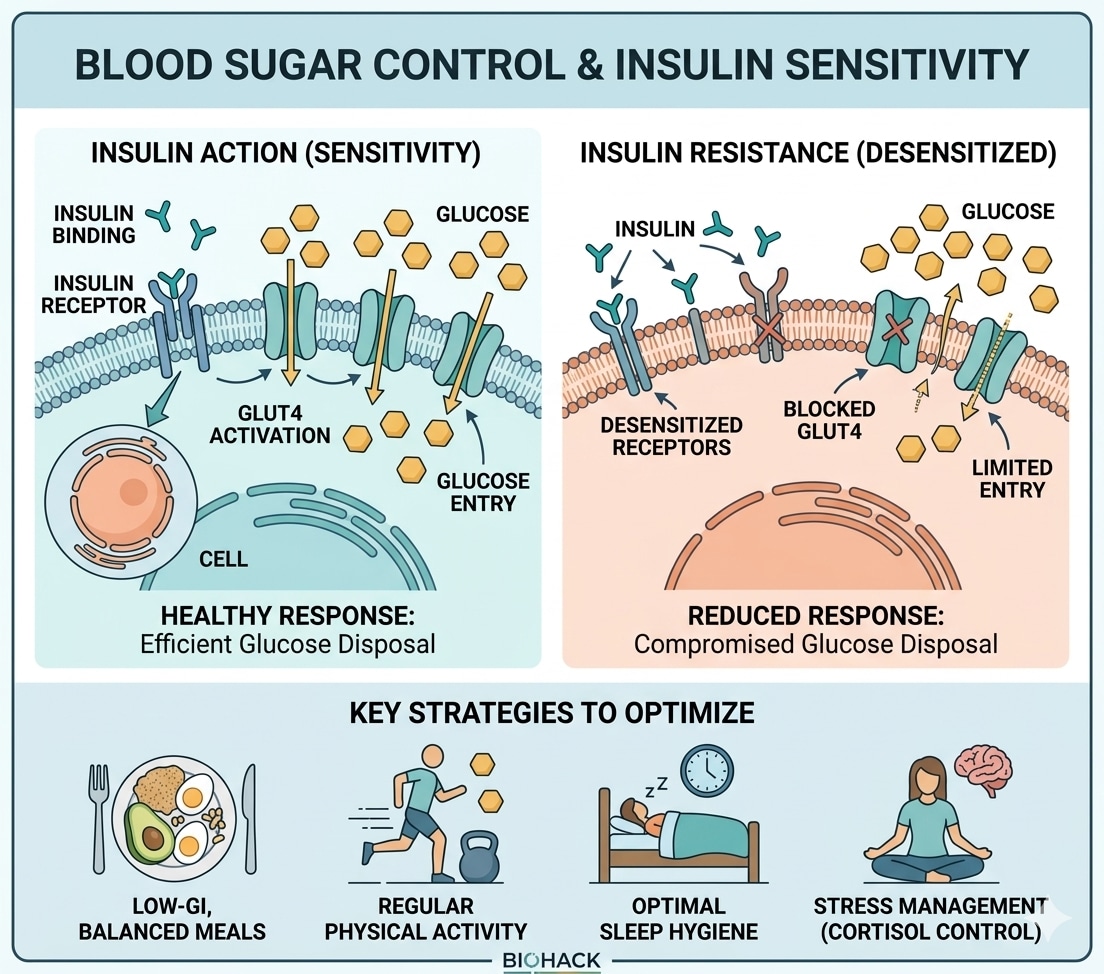
How Insulin and Glucose Normally Work
Whenever you consume food, dietary carbohydrates are broken down into glucose, which enters your bloodstream. Your pancreas detects this rise and immediately secretes insulin. Think of insulin as a biological key: it unlocks muscle, liver, and fat cells, allowing them to absorb glucose from the blood to be used for immediate cellular energy or stored safely as glycogen and triglycerides.
In a metabolically flexible, healthy adult, post-meal glucose might peak around 120–140 mg/dL and will return smoothly to a baseline of roughly 80–100 mg/dL within two to three hours.
However, over years or decades, an excess of calories, physical inactivity, chronic low-grade inflammation, and poor sleep can severely blunt the cells' responsiveness to this "key." This is insulin resistance. To compensate, the pancreas simply produces more insulin. For a long time, this sheer volume of insulin keeps blood sugar levels appearing normal on basic tests, but the underlying machinery is straining. Eventually, the pancreas fatigues, glucose remains elevated between meals, visceral fat accumulates, and the American Diabetes Association (ADA) thresholds for prediabetes are crossed.
The critical insight: Elevated fasting glucose is a late-stage alarm bell. Tracking fasting insulin and HOMA-IR can alert you to trouble years in advance.
Tracking Glucose and Insulin: What to Actually Measure
Instead of getting lost in a sea of medical cutoffs, focus on tracking these specific markers to understand your metabolic trajectory:
- Fasting Plasma Glucose
- Optimal: Under 100 mg/dL (metabolically healthy adults often sit between 80–95 mg/dL).
- Action Threshold: 100–125 mg/dL indicates prediabetes; ≥126 mg/dL on two occasions confirms diabetes per ADA diagnostic criteria.
- Hemoglobin A1c (HbA1c)
- Optimal: Under 5.7% (many healthy adults range from 5.0–5.4%).
- Action Threshold: 5.7–6.4% indicates prediabetes; ≥6.5% indicates diabetes. This marker shows your average blood sugar over the past 3 months.
- Fasting Insulin & HOMA-IR
- Optimal: Fasting insulin around 2–6 µIU/mL; HOMA-IR between 0.5–1.5.
- Action Threshold: A HOMA-IR consistently above 2–3 strongly suggests active insulin resistance, catching dysfunction well before glucose levels spike.
- Triglyceride-to-HDL Ratio
- Optimal: Triglycerides under 100 mg/dL with HDL above 50 mg/dL (ratio under 2:1).
- Why it matters: An elevated TG:HDL ratio on a standard lipid panel is one of the most accessible, widely available early markers of insulin resistance.
- CGM Time-in-Range (TIR)
- Optimal Target: At least 70% of daily readings falling between 70–180 mg/dL, according to ADA standards of care. Pay special attention to minimizing severe post-meal spikes and nocturnal variability.
Note: For individuals already diagnosed with diabetes, generalized targets may be adjusted—especially in older populations. Always align your personal goals with your prescribing physician.

Periodic fingerstick or CGM data reveals exactly which meals, exercise patterns, and sleep habits move your glucose — turning vague advice into a personalized protocol.
Image source: Unsplash.What Drives Insulin Resistance?
Insulin resistance is rarely the fault of a single bad habit. It typically emerges when multiple lifestyle factors push your biology in the wrong direction simultaneously:
- Visceral Adiposity (Excess Belly Fat): Fat tissue packed tightly around the liver and abdominal organs isn't just inert storage; it's hormonally active. It releases inflammatory cytokines that directly impair insulin action. Even a 5–10% weight reduction dramatically improves this.
- Physical Inactivity: Skeletal muscle is your body's largest "glucose sink." A sedentary lifestyle rapidly shrinks your muscle's capacity to absorb circulating sugar.
- Ultra-Processed Diets: High-frequency consumption of refined carbohydrates, liquid sugars, and heavily processed foods creates violent blood sugar spikes, forcing a chronic overproduction of insulin.
- Sleep Deprivation: Regularly getting less than 7 hours of sleep violently disrupts metabolic hormones. It spikes cortisol, suppresses the satiety hormone leptin, and measurably worsens glucose tolerance in a matter of days. You can explore the hormonal mechanics via the NIH overview of circadian biology.
- Chronic Stress: Relentless psychological stress keeps cortisol chronically elevated, which signals the liver to produce more glucose while simultaneously making cells resistant to insulin.
The silver lining: Because these systems are heavily interconnected, improving just one lever automatically aids the others. Better sleep reduces junk-food cravings; consistent exercise deepens your sleep quality; and stabilized blood sugar dramatically improves your daily energy levels.
Evidence-Based Lifestyle Interventions
Diet Composition and Quality
Prioritize Viscous Fiber: A meta-analysis of randomized clinical trials demonstrates that consuming 10–15 grams of soluble fiber daily can reduce HbA1c by ~0.5% and lower fasting glucose by roughly 18 mg/dL.
- Practical sources: Lentils, black beans, oats, psyllium husk, chia seeds, and cruciferous vegetables. Fiber acts as a biological sponge, slowing gastric emptying and dramatically blunting post-meal sugar spikes.
Protein and Healthy Fats: Securing adequate protein at every meal (25-35g) promotes satiety, preserves precious muscle mass, and slows the digestion of accompanying carbohydrates. Pairing this with healthy fats (extra-virgin olive oil, avocados, almonds) further flattens the metabolic curve.
Carb Quality Over Complete Elimination: You do not need to eliminate carbohydrates, but you must upgrade them. Swapping high-glycemic foods (white bread, sodas, pastries) for low-glycemic, intact foods (quinoa, sweet potatoes, legumes) results in vastly smaller insulin requirements. Both the Mediterranean and DASH diets leverage this exact mechanism to prevent diabetes.
Meal Timing and Intermittent Fasting
Early Time-Restricted Eating (TRE): Human metabolism is optimized to process food earlier in the day. Concentrating your calories into an earlier window—for example, eating a robust breakfast and finishing dinner by 6 PM—measurably improves insulin sensitivity. Late-night eating, conversely, clashes with rising melatonin levels, significantly worsening glucose tolerance.
Intermittent Fasting (IF): Protocols like 16:8 daily fasting or 5:2 patterns successfully improve glucose markers, primarily by naturally reducing overall caloric intake. If you adopt IF, prioritize the timing (front-loading your calories to the morning/afternoon) rather than obsessing over the exact duration of the fast.
Exercise: Aerobic vs. Resistance
Movement manages blood sugar through two completely distinct pathways: immediate contraction-induced glucose uptake (which doesn't even require insulin) and the long-term building of mitochondrial density.
- Aerobic Exercise: Brisk walking, cycling, or swimming directly lowers fasting glucose. The Physical Activity Guidelines for Americans strongly recommend a minimum of 150 minutes of moderate-intensity cardio per week.
- Resistance Training: Lifting weights expands the size of your "glucose sink." Network meta-analyses continually rank heavy resistance training as a premier intervention for lowering HOMA-IR. Aim for 2–3 full-body sessions weekly.
- The Post-Meal Walk: Simply walking for 10–15 minutes immediately after a heavy meal is one of the most underrated, highly effective biological hacks for blunting an acute glucose spike.
Sleep and Stress
- Sleep Optimization: Chronic short sleep creates an environment that mimics early prediabetes. Aim for 7–9 hours of high-quality sleep with a consistent wake-time. If you frequently wake unrefreshed or snore loudly, get evaluated for Obstructive Sleep Apnea (OSA)—a massive, silent driver of severe insulin resistance.
- Stress Management: Implement brief, daily "down-regulation" practices. Just 5 minutes of slow, controlled breathing (5–6 breaths per minute) or a brief walk outdoors without a phone can measurably lower acute cortisol and adrenaline, improving insulin action.
Putting It Together: A Daily Routine
How does this look in practice? Here is a scientifically optimized daily template:
- Morning (7:00 AM): Get bright outdoor sunlight in your eyes within 30 minutes of waking. Eat a high-protein, high-fiber breakfast (e.g., a 3-egg omelet with spinach, or Greek yogurt with chia seeds and berries). If you prefer fasted workouts, do them before this meal.
- Midday (1:00 PM): A balanced lunch featuring lean protein, a massive serving of non-starchy vegetables, a modest portion of intact whole grains, and a healthy fat. Follow this immediately with a 10-minute walk.
- Afternoon (3:30 PM): Stand up or stretch every hour. If genuinely hungry, snack on a handful of raw almonds or walnuts rather than a refined carbohydrate bar.
- Evening (6:30 PM): Eat an earlier, lighter dinner. Prioritize protein and vegetables, keeping carbohydrates minimal. Take a leisurely 15-minute stroll around the neighborhood afterward.
- Wind-down (9:00 PM): Dim overhead lights to signal melatonin production. No caloric intake. Go to bed by 10:30 PM to secure 8 solid hours of sleep.
Decision Guide: When to Test or Seek Help
Use this simple, step-by-step flow if you are experiencing symptoms like persistent fatigue, frequent urination, unquenchable thirst, or stubborn weight gain:
- Request standard labs. Ask your doctor for a fasting glucose, HbA1c, fasting insulin, and a comprehensive lipid panel.
- Interpret your data.
- Optimal range: Keep up the foundational habits. Re-test annually.
- Prediabetes range (glucose 100–125 mg/dL or HbA1c 5.7–6.4%): Escalate your lifestyle interventions. Tighten carbohydrate quality, ensure 150+ minutes of combined exercise weekly, and aim for a 5% body weight reduction if applicable. Re-test in 3–6 months.
- Diabetes range (glucose ≥126 mg/dL or HbA1c ≥6.5%): Consult your clinician for a formal diagnosis and a structured treatment plan, which may include pharmacology.
- Adjust based on feedback. If aggressive lifestyle changes over 6 months do not shift your markers, escalate your clinical care. Hidden drivers like thyroid dysfunction, undiagnosed sleep apnea, or genetic factors may require medical intervention.
Supplements and Medications
Treat supplements as minor boosts, never as foundational fixes. Always consult your doctor before starting them, especially if you are on current medications.
- Metformin: The gold-standard, first-line prescription medication for type 2 diabetes. It works by reducing the amount of glucose the liver pumps out and slightly improving peripheral insulin sensitivity. It boasts decades of robust safety data.
- Berberine: A bioactive plant compound backed by meta-analyses showing reductions in fasting glucose (~8 mg/dL) and HbA1c (~0.4–0.5%). Typical dosing is 500mg taken 2-3 times daily with meals. Since it is largely unregulated in the supplement market, brand quality matters immensely.
- Cinnamon (Ceylon): Can yield minor reductions in fasting glucose when used daily, but the clinical effects are minimal compared to diet and exercise. (Note: Always choose Ceylon cinnamon to avoid the liver toxicity associated with high doses of Cassia cinnamon).
- Chromium: Despite heavy marketing, major medical guidelines note the evidence is too weak and inconsistent to recommend for glucose control.
Comparing Interventions at a Glance
| Intervention | Effect on Glucose & Insulin Sensitivity | Strength of Evidence |
|---|---|---|
| Fiber-rich diet | HbA1c ↓ ~0.4–0.5%; significantly smaller post-meal spikes | Very Strong (RCTs) |
| Mediterranean pattern | Lower diabetes risk; drastically improved insulin sensitivity | Very Strong |
| Replacing refined carbs | Flattens glucose excursions; lowers overall insulin demand | Very Strong |
| Weight loss (5–10%) | HbA1c ↓ ~0.5–1.0%; massive gains in insulin sensitivity | Very Strong (DPP, DiRECT) |
| Aerobic exercise | Fasting glucose ↓; immediate insulin sensitivity ↑ | Very Strong |
| Resistance training | HOMA-IR ↓; permanent increase in glucose disposal capacity | Strong |
| Combined exercise | Yields the largest combined drops in glucose and HOMA-IR | Strong |
| Sleep optimization | Reverses acute, sleep-deprivation-induced insulin resistance | Moderate (Strong mechanism) |
| Early time-restricted eating | Lowers glucose peaks; reduces HbA1c in a calorie deficit | Emerging |
| Berberine | HbA1c ↓ ~0.4–0.5%; HOMA-IR ↓ | Good (Meta-analyses) |
| Cinnamon (Ceylon) | HbA1c ↓ ~0.3–0.5%; modest fasting glucose ↓ | Moderate |
| Chromium | Negligible impact for most users | Weak / Inconsistent |
Key Takeaways
Achieving stable blood sugar isn't about rigid perfection; it's about compounding consistency. The synergistic effect of a fiber-forward diet, progressive resistance and aerobic training, early time-restricted eating, prioritized sleep, and a 5–10% reduction in body weight will drastically outperform any supplement on the market.
Track the biomarkers that actually matter—fasting glucose, HbA1c, and fasting insulin—make targeted adjustments, and always work alongside a qualified clinician when your numbers fall out of range.
For a deeper dive into optimizing your daily energy pathways, explore our comprehensive guides on Metabolic Health, How Cellular Metabolism Works, and Beating Chronic Fatigue.
Scientific References:
- Centers for Disease Control and Prevention. National Diabetes Statistics Report. cdc.gov
- American Diabetes Association. Standards of Care in Diabetes — Diagnosis and Classification. diabetesjournals.org
- American Diabetes Association. Standards of Care in Diabetes — Glycemic Goals and Hypoglycemia. diabetesjournals.org
- National Institute of Diabetes and Digestive and Kidney Diseases. Diabetes — Symptoms, Causes, and Treatment. niddk.nih.gov
- National Institute of General Medical Sciences. Circadian Rhythms — Fact Sheet. nigms.nih.gov
- U.S. Department of Health and Human Services. Physical Activity Guidelines for Americans, 2nd Edition. health.gov
- Diabetes Prevention Program Research Group. Reduction in the Incidence of Type 2 Diabetes with Lifestyle Intervention or Metformin. pubmed.ncbi.nlm.nih.gov
- Lean ME, Leslie WS, et al. Primary Care–Led Weight Management for Remission of Type 2 Diabetes (DiRECT). thelancet.com